3D Planning for a Complex Bentall Procedure After Arterial Switch
Patient background
A 33-year-old male with a history of complete transposition of the great arteries (TGA) underwent an arterial switch operation (ASO) with VSD and PDA closure at the age of 3. The postoperative course was uneventful, with a residual small VSD and mild aortic regurgitation.
Over time, progressive dilation of the neo-aortic root developed, ultimately reaching 63 mm on echocardiography, with associated mild–moderate aortic insufficiency.
Clinical scenario
The patient presented for evaluation of surgical repair. The team considered two main options:
David procedure (valve-sparing root replacement)
Bentall operation (composite graft with aortic valve replacement)
The decision hinged on the precise anatomical assessment of the aortic root, coronary anatomy, and spatial relations after the previous ASO — where the great vessels are translocated, altering standard anatomy.
Imaging & Data Acquisition
CT angiography was performed 3 days prior to surgery.
Images were processed in 3D Slicer using a custom extension I developed, which integrates an nnU-Net–based automatic segmentation pipeline.
This extension computes parameters not available in default workflows, including:
Aortic root rotation angle (due to post-ASO distortion)
Coronary ostia distance to annulus
Relation between aortic root & pulmonary trunk
Graft sizing recommendations
Coronary take-off angles
Sinotubular junction diameter and eccentricity
Clearance measurements for coronary button reimplantation
3D Modelling Workflow
Segmentation – Fully automated, completed in ~20 minutes.
Design & surgical planning – 20 minutes, including annotation of critical landmarks.
3D printing – SLA technology on a Formlabs 3B printer using surgical-grade, sterilizable resin. Print time: ~8 hours.
Post-processing – 1 hour, including cleaning, curing, and sterilization.
Surgical Impact
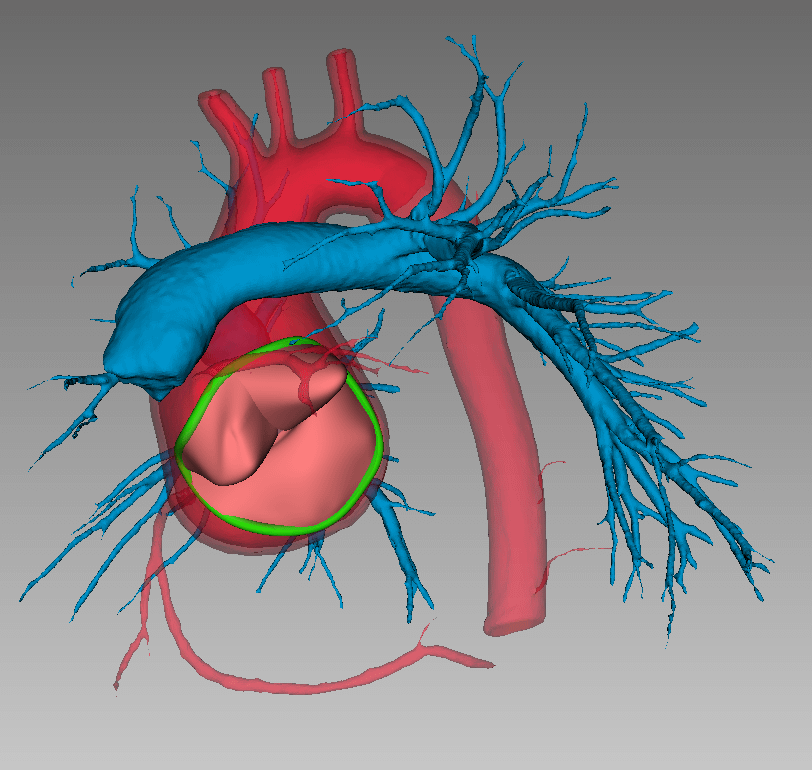
The virtual and printed 3D models provided crucial insights:
Confirmed rotational distortion of the neo-aortic root from prior ASO.
Assessed the relative positions of the neo-aorta and main pulmonary artery trunk, influencing the approach to vessel separation.
Allowed selective dissection — only the right pulmonary artery was separated from the trunk; the left remained intact, avoiding unnecessary patch reconstruction.
Helped determine that there was sufficient space for the aortic conduit after aneurysm resection.
Guided coronary button positioning to avoid tension or kinking.
Based on these findings, the team proceeded with a Bentall operation, as the root dilation and annular geometry made valve preservation (David procedure) less favorable.

Conclusions
This case demonstrates how integrating customized 3D imaging workflows into congenital and reoperative cardiac surgery can:
Provide quantitative as well as qualitative anatomical data
Reduce operative uncertainty in complex anatomies
Enable a more conservative dissection strategy
Potentially shorten operative time and avoid unnecessary reconstructions