Surgical Management of Secondary Localized Tracheomalacia Caused by Straight Back Syndrome — Case Report —
Patient background
A 9.5-year-old girl with spastic tetraparesis and somatomental retardation, a consequence of intrauterine injury, was admitted to the Pediatric Intensive Care Unit following successful resuscitation. Her medical history revealed multiple episodes of opisthotonus and apnea since the age of two, initially misinterpreted as affective apnea due to emotional triggers. Despite pharmacologic therapy and PEG placement for recurrent respiratory infections, her episodes became more frequent and severe, ultimately leading to life-threatening airway obstruction.
Clinical scenario
The patient was diagnosed with Straight Back Syndrome, a rare deformity where the sternum and thoracic spine are abnormally close, resulting in a markedly decreased anteroposterior chest diameter.
This configuration caused compression of the trachea and mediastinal structures, leading to secondary localized tracheomalacia and dynamic airway collapse, mimicking neurological episodes.
Key pathology: Tracheal narrowing by ~70% in the lower third of the trachea.
Symptoms: Dyspnea, episodic cyanosis, opisthotonic posture.
Complication: Chronic airway obstruction due to bony compression.
Imaging & Data Acquisition
High-resolution CT-angiography was performed to reconstruct the osseous thorax, with special focus on the sternumand thoracic vertebrae.
Subsequently, the trachea and great vessels (aorta and pulmonary arteries) were also segmented and reconstructed in 3D to fully understand the anatomical compression.
AP chest diameter: 16 mm at its narrowest point.
Findings: Flattened thoracic cage, steeply oriented ribs, and anteroposterior tracheal compression.
Purpose: To precisely quantify the skeletal geometry and design a patient-specific surgical solution.
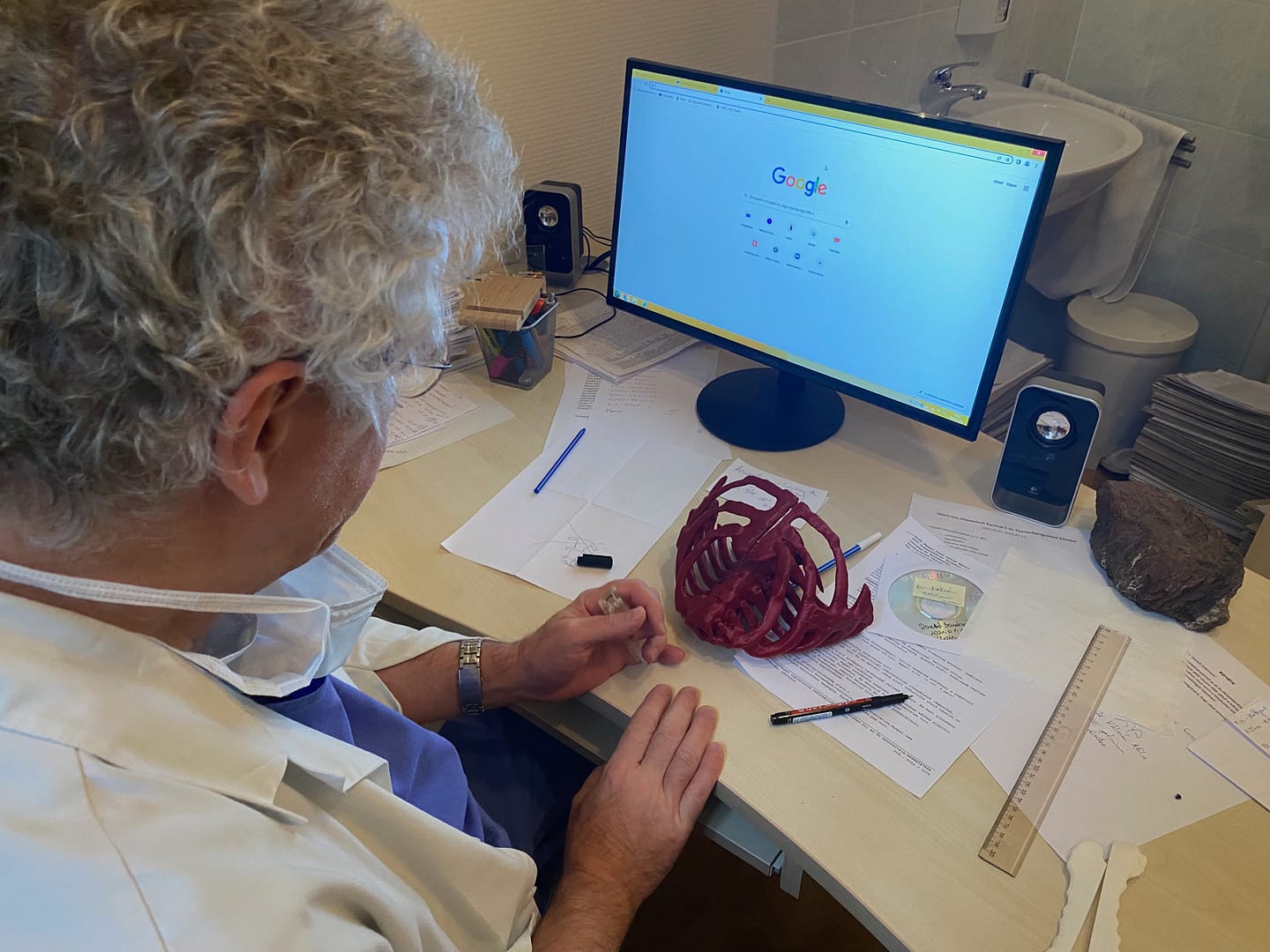
3D Modelling Workflow
Using the high-resolution CT data, a dimensionally accurate 3D model of the sternum was generated.
The sternum was virtually divided along the midline.
A custom-designed implant was modeled to separate the two halves by an optimal distance, based on preoperative biomechanical calculations, to relieve tracheal compression.
The device was machined using a 5-axis milling system rather than 3D printing, ensuring high precision.
Material: Polyether ether ketone (PEEK), chosen for its excellent biocompatibility, rigidity, and sterilizability.

Surgical Impact
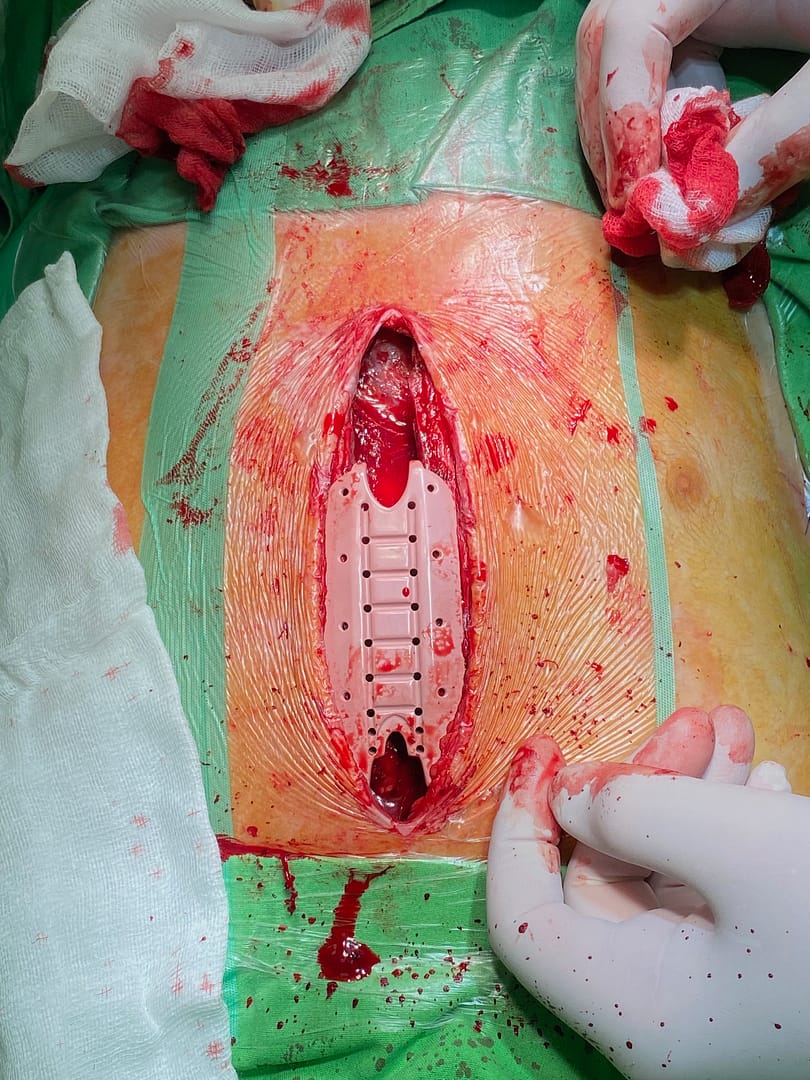
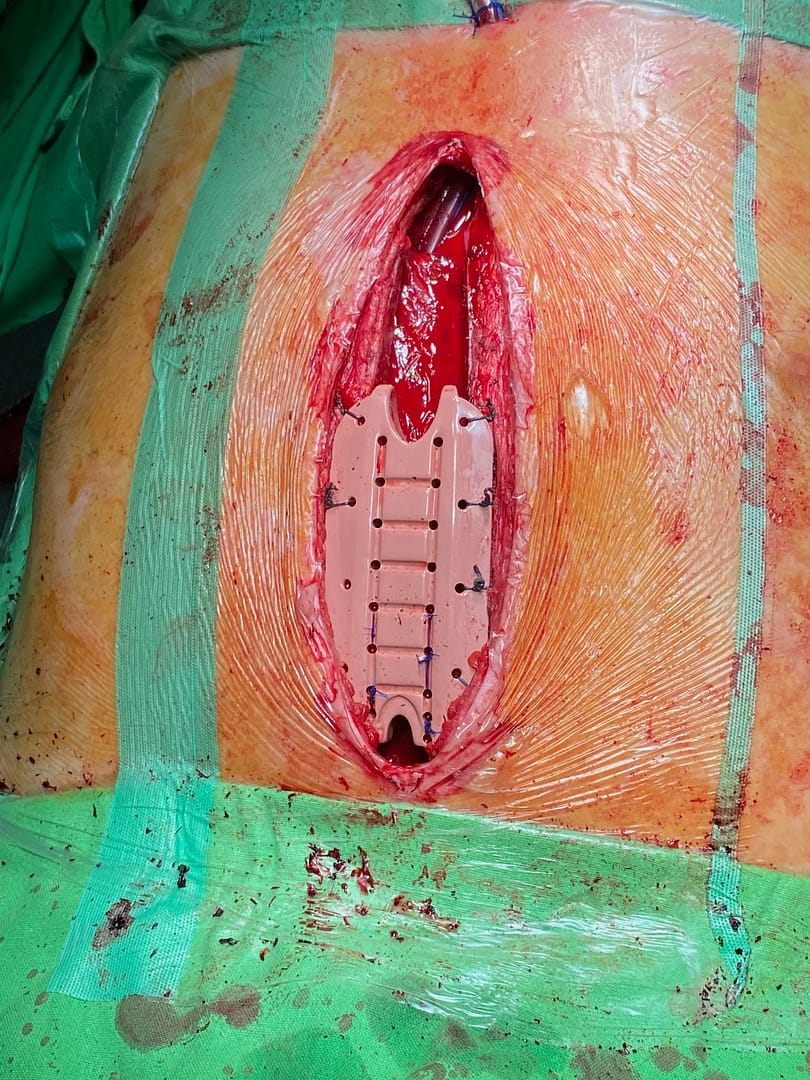
During surgery, the sternum was carefully divided, and the tissues behind it were released to allow decompression.
The custom sternum-spreading implant was then inserted and secured bilaterally using 0 Prolene or 0 Vicryl monofilament sutures through pre-designed fixation holes.
Design characteristics:
The implant’s lateral flanges conformed perfectly to the bony contours of the sternum.
It provided additional stability by acting as a socket-like support that enveloped the bone edges.
Because it was patient-specific, intraoperative adaptation was unnecessary.
Intraoperative findings:
Tracheal decompression was immediately evident.
No hemodynamic instability occurred during the procedure.
Postoperative outcome:
Bronchoscopic evaluation confirmed marked tracheal dilatation.
The patient’s initial symptoms — particularly dyspnea and episodic airway collapse — completely resolved.
No recurrence of airway obstruction was observed during follow-up.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Conclusions
This case demonstrates how advanced 3D medical technologies can offer novel, previously unavailable surgical solutions for complex, anatomically constrained problems.
By integrating high-resolution imaging, 3D modeling, and precision manufacturing, a custom sternum expansion implant was successfully created and implanted, restoring airway patency and resolving the patient’s respiratory symptoms.
Such technology-driven approaches transcend traditional surgical intuition, opening new dimensions in patient-specific treatment planning and intraoperative precision, and represent a promising direction in future personalized thoracic surgery.