Unifocalization in MAPCA Surgery Supported by Patient-Specific 3D Modeling
Patient background
The patient was diagnosed with pulmonary atresia with ventricular septal defect (PA/VSD) and major aortopulmonary collateral arteries (MAPCAs). The pulmonary circulation was supplied primarily through multiple collateral vessels, while the native pulmonary arteries were hypoplastic. This complex anatomy necessitated a staged surgical approach, beginning with palliation and followed by unifocalization.
Clinical scenario
- The first step in the surgical series consisted of palliative treatment to ensure sufficient pulmonary blood flow and stabilize the patient.
- The second step was the unifocalization procedure, where the collateral arteries were mobilized and connected to the native pulmonary arteries to establish a functional and unified pulmonary circulation.
Given the highly variable and intricate anatomy of MAPCAs, a reliable roadmap was essential to support intraoperative navigation.
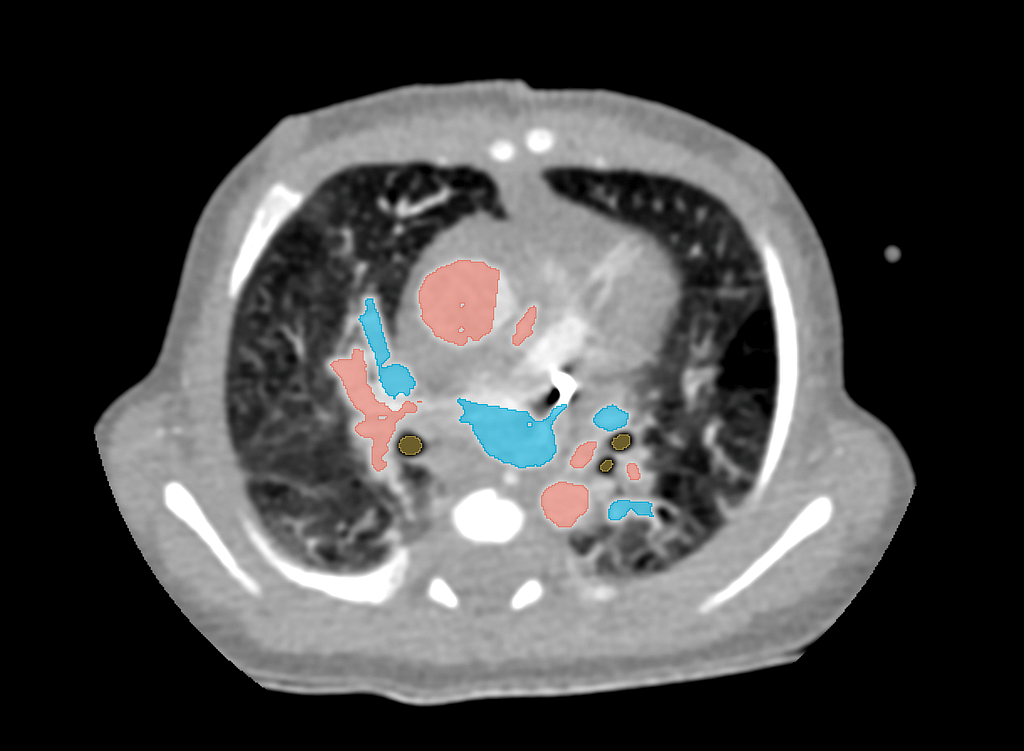
Imaging & Data Acquisition
One week prior to surgery, the patient underwent a high-resolution CT angiography. The dataset allowed for segmentation of:
the collateral arteries (MAPCAs),
the aorta,
the native pulmonary branches, and
the trachea as a spatial reference.
This detailed anatomical map formed the basis for the subsequent 3D modeling.
3D Modelling Workflow
From the segmented CT angiography, a patient-specific 3D model was generated. Special attention was given to differentiating the collateral vessels from the native pulmonary arteries, providing clarity in their origin, course, and connections.
The model was then:
Processed for 3D printing using sterilizable biocompatible polymer,
Printed at a 1:1 anatomical scale,
Sterilized for intraoperative use.
This workflow ensured that the model could be directly used as a surgical roadmap during the unifocalization procedure.
Surgical Impact
During surgery, the 3D-printed model served as a sterile anatomical guide, allowing the surgical team to precisely locate each collateral vessel. The tactile and visual reference greatly facilitated dissection, reduced operative uncertainty, and enhanced the precision of the unifocalization process.
By mapping the vessels directly onto the model, the team was able to shorten the intraoperative search time and achieve a more complete reconstruction of the pulmonary vasculature.

Conclusions
The integration of patient-specific 3D modeling into MAPCA surgery provided significant advantages. The printed, sterilized model functioned as a real-time anatomical map, directly improving surgical orientation and efficiency.
This case demonstrates how advanced imaging, segmentation, and 3D printing can transform the management of highly complex congenital heart defects, ultimately supporting better surgical outcomes and patient safety.